Male to Female (MTF) Trans-feminine Hormone Therapy
The aim of Feminizing Hormone Therapy (FHT) is to make a person’s body more like the gender they identify with. This means using female hormones to help them look and feel more like a woman. It’s meant to reduce the distress they feel because their body doesn’t match their gender identity (Coleman et al., 2012; Hembree et al., 2017).

Before starting feminizing hormone therapy, certain conditions need to be met (Hembree et al., 2017):
- The person must have persistent and well-documented gender dysphoria or incongruence.
- They need to be able to understand and agree to the treatment after being fully informed.
- If they’re not of legal adult age, they should meet criteria appropriate for adolescents.
- Any mental or medical health issues they have should be reasonably controlled.
Before starting feminizing hormone therapy, it’s important to evaluate the person’s health (Hembree et al., 2017):
- Doctors follow guidelines to check for medical conditions that might get worse with the therapy.
- Using hormones without supervision is strongly discouraged, and efforts should be made to reduce or quit tobacco use.
- The healthcare provider asks about personal and family medical history, especially looking for cancers affected by hormones (prostate cancer/ breast cancer), liver problems, heart disease, and blood clot risks.
- They might do tests like checking cholesterol, blood sugar, blood counts, liver function, and hormone levels.
- They also check vaccination history (HPV vaccination), look for substance use or infections like HIV and STI, and discuss fertility plans and safe treatments.
The way feminizing hormone therapy is done can vary based on where you live, what medicines are available, and how much they cost (Wylie et al., 2016). Usually, it involves taking drugs to reduce testosterone (antiandrogens and GnRH analogs) and also taking estrogen to stop testosterone production and make the body more feminine.
Different types of Feminizing Hormone Therapy:
- Estrogen reduces testosterone production from the testes and helps develop feminine physical features. The most common estrogen used is 17b-Estradiol, which might have a lower risk of blood clots (thromboembolism) compared to other synthetic estrogens (Canonico et al., 2008; Ott et al., 2010).
- Antiandrogens block the effects of male hormones and can also lower testosterone levels. Spironolactone and cyproterone acetate are common antiandrogens used.
- Spironolactone acts on hormone receptors and can decrease testosterone production (mineralocorticoid receptor blocker), but it may cause high potassium levels (hyperkalemia) (Deedwania & Mather, 2014).
- Cyproterone acetate is a hormone blocker (progestin with androgen-blocking features) but can have side effects like liver problems (hepatotoxicity), depression, and certain brain related effect (multifocal meningiomas) (Gil et al., 2011; Gazzeri et al., 2007).
- 5a-Reductase inhibitors like finasteride can also be used to block the conversion of testosterone to another potent male hormone (dihydrotestosterone), but they may affect mood negatively (Spack, 2013). Androgen receptor antagonists like bicalutamide don’t lower testosterone levels and can harm the liver (hepatotoxic) (Manson et al., 2013). So, drugs like Finasteride and Bicalutamide are not the first choice for therapy.
- GnRH analogs (e.g. leuprolide, goserelin, and histrelin) lower the production of certain hormones from the brain (luteinizing hormone and follicle-stimulating hormone), which decreases testosterone levels. When used with estrogen, GnRH analogs can effectively lower testosterone with fewer side effects (Dittrich et al., 2005). They can be considered for transgender individuals who can’t use antiandrogens or need a lower dose of estrogen, but they’re not widely used due to their cost.
- Progestins are sometimes used in feminizing hormone therapy to improve breast development and mood, but their role is uncertain. Studies on their effects are limited, and they’re not typically recommended as part of standard treatment (Wierckx et al., 2014).
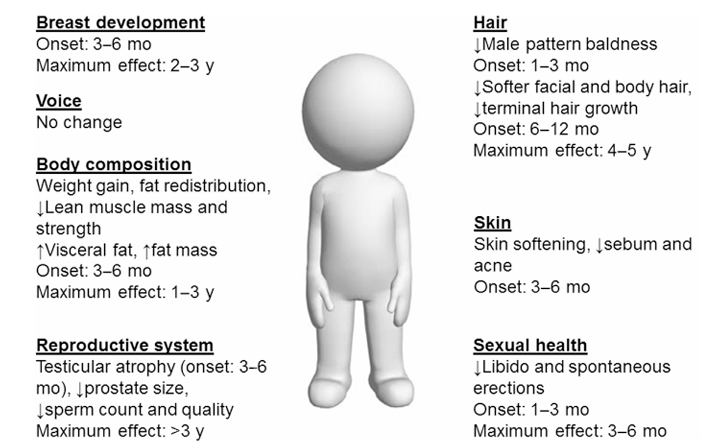
Feminizing Effects:
References:
- Coleman E, Bockting W, Botzer M, et al. Standards of care for the health of trans sexual, transgender, and gender-nonconforming people, version 7. Int J Trans gend 2012;13(4):165–232.
- Canonico M, Plu-Bureau G, Lowe GD, et al. Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: systematic review and meta-analysis. BMJ 2008;336(7655):1227–31.
- Deedwania PC, Mather PJ. Drug & device selection in heart failure. New Delhi (India): JP Medical Ltd; 2014.
- Dittrich R, Binder H, Cupisti S, et al. Endocrine treatment of male-to-female trans sexuals using gonadotropin-releasing hormone agonist. Exp Clin Endocrinol Dia betes 2005;113(10):586–92.
- Gazzeri R, Galarza M, Gazzeri G. Growth of a meningioma in a transsexual pa tient after estrogen–progestin therapy. N Engl J Med 2007;357(23):2411–2.
- Gil M, Oliva B, Timoner J, et al. Risk of meningioma among users of high doses of cyproterone acetate as compared with the general population: evidence from a population-based cohort study. Br J Clin Pharmacol 2011;72(6):965–8.
- Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2017;102(11):3869–903.
- Manson JE, Chlebowski RT, Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women’s Health Initiative randomized trials. JAMA 2013;310(13):1353–68.
- Ott J, Kaufmann U, Bentz E-K, et al. Incidence of thrombophilia and venous thrombosis in transsexuals under cross-sex hormone therapy. Fertil Steril 2010; 93(4):1267–72.
- Spack NP. Management of transgenderism. JAMA 2013;309(5):478–84.
- Wierckx K, Gooren L, T’sjoen G. Clinical review: Breast development in trans women receiving cross-sex hormones. J Sex Med 2014;11(5):1240–7.
- Wylie K, Knudson G, Khan SI, et al. Serving transgender people: clinical care considerations and service delivery models in transgender health. Lancet 2016;388(10042):401–11.